






















This material is intended for people without medical education who want to know more about osteochondrosis than is written in popular publications and on the websites of private clinics.Patients ask doctors of various specialties questions that characterize a complete misunderstanding of the topic of osteochondrosis.Examples of such questions include: “why does my osteochondrosis hurt?”, “congenital osteochondrosis was discovered, what should I do?”Perhaps the apotheosis of such illiteracy can be considered a fairly common question: “Doctor, I have initial signs of chondrosis, how scary is it?”This article is intended to structure the material about osteochondrosis, its causes, manifestations, methods of diagnosis, treatment and prevention, and answer the most frequently asked questions.Since all of us, without exception, are patients with osteochondrosis, this article will be useful to everyone.
How is the intervertebral disc structured?
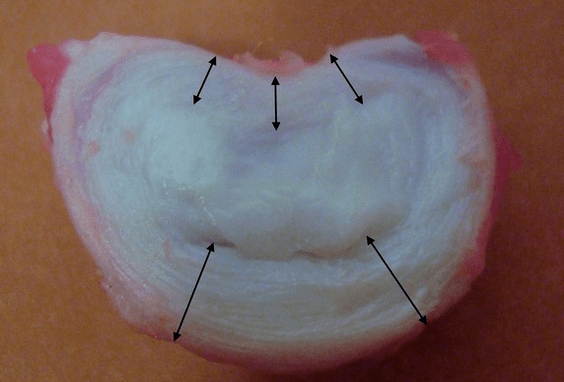
Each intervertebral disc consists of two different sections:
- outer fibrous ring, consisting of dense fibers covering the disc from the outside around the perimeter;
- the internal elastic component is the nucleus pulposus.
The fibers of the annulus fibrosus are very dense and elastic.Over the years, elasticity is lost, and by the age of 60 the fibrous ring becomes rigid.Between the surface of each overlying and underlying vertebra and the disc itself there are so-called endplates, that is, the border zones between the vertebra and the disc.Due to these endplates, the vertebrae grow in height, and through them, the nucleus pulposus and tissues of the intervertebral disc are diffusely nourished by the diffusion method, since the cartilage of the disc is not supplied with blood or innervated.
Healthy intervertebral discs in a young person are capable of high metabolic rates.If you introduce contrast into a normal disk, then after 20 minutes it disappears from it.
Studies have shown that in an adult, the height of each intervertebral disc is approximately:
- 25% of the height of adjacent vertebrae in the cervical region;
- 20% in the chest;
- 33% in the lumbar.
That is, in the lumbar region the thickness of the discs is greatest, due to the greatest load.Laboratory studies have shown that a single healthy disc in a young person can withstand a static compressive load of up to 2.5 tons.At the age of 70, this figure decreases to 110 kg!That is, an “old and dried out disk” copes 22 times worse with transferring load to the sides and with maintaining increased pressure within the ring.
Why did this happen?Over time, the fibrous ring gradually wears out.It can no longer stretch, but only protrudes outward, beyond the disc, or breaks.The core stops transmitting and transforming vertical load into radial load.With age, stress gradually accumulates inside the discs, and their structure changes.If all these processes, taken in a separate disc, are transferred to the entire spinal column, then we get a condition called osteochondrosis in the clinic.Now we can begin to define.
What is osteochondrosis?
The name of the disease is scary when it is not clear.The medical suffix “-oz” means proliferation or enlargement of some tissue: hyalinosis, fibrosis.An example would be cirrhosis of the liver, when the connective tissue grows and the functional tissue, hepatocytes, decreases in volume.There may be an accumulation of pathological protein, or amyloid, which should not normally be present.This storage disease will then be called amyloidosis.There may be a significant enlargement of the liver due to fatty degeneration, which is called fatty hepatosis.
Well, it turns out that with intervertebral osteochondrosis, the cartilage tissue of the intervertebral discs increases in volume, because “chondros, χόνδρο” translated from Greek into Russian means “cartilage”?No, chondrosis, or, more precisely, osteochondrosis is not a storage disease.No true growth of cartilage tissue occurs in this case; we are only talking about a change in the configuration of the intervertebral cartilaginous discs under the influence of many years of physical activity, and we examined above what happens in each individual disc.The term “osteochondrosis” was introduced into the clinical literature by A. Hilderbrandt in 1933.
Osteochondrosis refers to dystrophic-degenerative processes, and is part of the normal, normal aging of intervertebral discs.None of us are surprised that the face of a 20-year-old girl will be slightly different from her face at the age of 70, but for some reason everyone believes that the spine, its intervertebral discs, do not undergo the same pronounced temporary changes.Dystrophy is a nutritional disorder, and degeneration is a violation of the structure of the intervertebral discs that follows a long period of dystrophy.
Causes of osteochondrosis and its complications
The main cause of uncomplicated, physiological osteochondrosis can be considered the way a person moves: upright walking.Man is the only species on earth that walks on two legs among all mammals, and this is the only way of locomotion.Osteochondrosis became the scourge of humanity, but we freed our hands and created civilization.Thanks to upright walking (and osteochondrosis), we not only created the wheel, the alphabet and mastered fire, but you can also sit at home in the warmth and read this article on your computer screen.
Humans' closest relatives, the higher primates - chimpanzees and gorillas, sometimes rise on two legs, but this method of movement is auxiliary for them, and most often they still move on four legs.In order for osteochondrosis to disappear, like intensive aging of the intervertebral discs, a person needs to change the way they move and remove the constant vertical load from the spinal column.Dolphins, killer whales and whales do not have osteochondrosis, and dogs, cows and tigers do not have it.Their spine does not take on long-term static and shock vertical loads, since it is in a horizontal state.If humanity goes to sea and the natural way of transportation is scuba diving, then osteochondrosis will be defeated.
Upright posture forced the human musculoskeletal system to evolve in the direction of protecting the cranium and brain from shock loads.But discs - elastic pads between the vertebrae - are not the only method of protection.A person has a springy arch of the foot, cartilage of the knee joints, physiological curves of the spine: two lordosis and two kyphosis.All this allows you not to “shake off” your brain even while running.
Risk factors
But doctors are interested in those risk factors that can be modified and avoid complications of osteochondrosis, which cause pain, discomfort, limited mobility and reduced quality of life.Let's consider these risk factors, which are so often ignored by doctors, especially in private medical centers.After all, it is much more profitable to constantly treat a person than to point out the cause of the problem, solve it, and lose the patient.Here they are:
- the presence of longitudinal and transverse flat feet.Flat feet cause the arch of the foot to stop springing, and the shock is transmitted upward to the spinal column without softening.Intervertebral discs experience significant stress and quickly collapse;
- overweight and obesity - needs no comment;
- improper lifting and carrying of heavy objects, with uneven pressure on the intervertebral discs.For example, if you lift and carry a bag of potatoes on one shoulder, then the intense load will fall on one edge of the disks, and it can be excessive;
- physical inactivity and a sedentary lifestyle.It was said above that it is during sitting that the maximum pressure on the discs occurs, since a person never sits straight, but always “slightly” bends;
- chronic injuries, slipping on ice, intense weightlifting, contact martial arts, heavy hats, hitting your head on low ceilings, heavy clothing, carrying heavy bags in your hands.
General symptoms
The symptoms that will be described below exist outside of localization.These are common symptoms and can exist anywhere.These are pain, movement disorders and sensory disturbances.There are also vegetative-trophic disorders, or specific symptoms, for example, urinary disorders, but much less frequently.Let's take a closer look at these signs.
Pain: muscle and radicular
Pain can be of two types: radicular and muscular.Radicular pain is associated with compression, or pressing of a protrusion or herniation of the intervertebral disc of the corresponding root at this level.Each nerve root consists of two portions: sensitive and motor.
Depending on where exactly the hernia is directed and what portion of the root has been compressed, there may be either sensory or motor disorders.Sometimes both disorders occur at once, expressed to varying degrees.Pain also belongs to sensory disorders, since pain is a special, specific feeling.
Radicular pain: compression radiculopathy
Radicular pain is familiar to many; it is called “neuralgia”.The swollen nerve root reacts violently to any shock, and the pain is very sharp, similar to an electric shock.She shoots either in the arm (from the neck) or in the leg (from the lower back).Such a sharp, painful impulse is called a lumbago: in the lower back it is lumbago, in the neck it is cervicago, a rarer term.Such radicular pain requires a forced, analgesic, or antalgic posture.Radicular pain immediately occurs when coughing, sneezing, crying, laughing, or straining.Any shock to the swollen nerve root causes increased pain.
Muscle pain: myofascial-tonic
But an intervertebral hernia or disc defect may not compress the nerve root, but when moving, injure nearby ligaments, fascia, and deep back muscles.In this case, the pain will be secondary, aching, permanent, stiffness in the back will occur, and such pain is called myofascial.The source of this pain will no longer be the nervous tissue, but the muscles.A muscle can respond to any stimulus in only one way: contraction.And if the stimulus is prolonged, the muscle contraction will turn into a constant spasm, which will be very painful.
A characteristic symptom of such secondary, myofascial pain will be increased stiffness in the neck, lower back or thoracic spine, the appearance of dense, painful muscle bumps - “rollers” next to the spine, that is, paravertebral.In such patients, back pain intensifies after several hours of “office” work, with prolonged immobility, when the muscles are practically unable to work and are in a state of spasm.
Sensory disorders
If a protrusion or hernia, or a spasmodic muscle presses the sensitive portion of the nerve root, then various sensory disorders occur.They may be accompanied by pain, or they may occur separately, after the pain has already passed.There are also completely painless forms of sensory disorders, but rarely.
Many people know the numbness of the tips of the fingers and toes (hypoesthesia or complete anesthesia), decreased sensitivity of the skin in the form of long stripes, of the radicular type.Sometimes paresthesia, or formication, a sensation of “crawling goosebumps” occurs.Most often, sensitivity disorders occur in the feet, and tips of the fingers and toes.Sensory disorders are quite unpleasant, but sensory disorders do not make a person disabled, but motor disorders may well lead to this.
Motor disorders in the periphery
If a motor neuron or axons that are part of the motor portion of a nerve are affected, then either weakness in the muscle or its complete immobility occurs.In the second case we are talking about complete paralysis, and in the first case - about paresis.Paresis is partial paralysis when the muscle does not work at full strength.
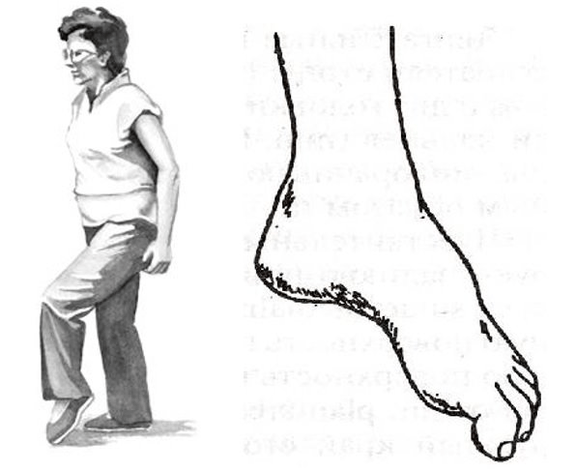
Most often, such disorders appear in the legs, with protrusions and hernias of the lumbar spine.There lie motor structures that innervate the muscles of the lower leg and foot.Therefore, with advanced, complicated lumbar osteochondrosis, the foot may spank.It turns inward, the person is forced to raise his leg high in order to step with the spanking foot, this is called steppage, “cock gait.”
But the whole danger of movement disorders is that they can be isolated and not accompanied by pain.And if a person “does not have pain,” then he may not get to the doctor in a timely manner.Therefore, it is so important for patients with progressive protrusions and hernias, for example, of the lumbar region, to periodically walk on their toes and heels, and monitor the work of their muscles.
Local symptoms: main signs
Let us now consider specific symptoms and syndromes characteristic of cervical, thoracic, and lumbar osteochondrosis.Let's go from top to bottom, from the cervical region down, through the thoracic region, to the lumbosacral region.
Diagnosis of osteochondrosis
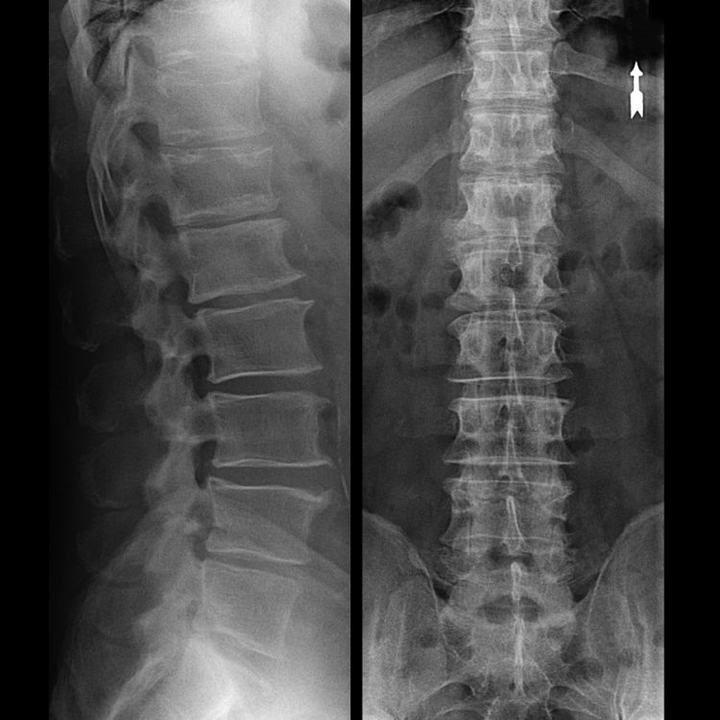
In typical cases, osteochondrosis of the cervical and cervical-thoracic spine occurs as described above.Therefore, the main stage of diagnosis was and remains the identification of the patient’s complaints, establishing the presence of concomitant muscle spasm using simple palpation of the muscles along the spinal column.Is it possible to confirm the diagnosis of osteochondrosis using x-ray examination?
An “X-ray” of the cervical spine, and even with functional tests for flexion and extension, does not show cartilage, since their tissue transmits X-rays.Despite this, based on the location of the vertebrae, one can draw general conclusions about the height of the intervertebral discs, the general straightening of the physiological curvature of the neck - lordosis, as well as the presence of marginal growths on the vertebrae with prolonged irritation of their surfaces by fragile and dehydrated intervertebral discs.Functional tests can confirm the diagnosis of instability in the cervical spine.
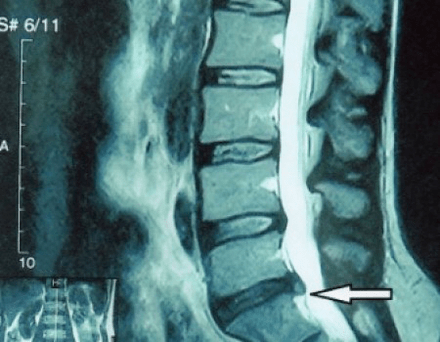
Since the discs themselves can only be seen using CT or MRI, magnetic resonance and x-ray computed tomography are indicated to clarify the internal structure of cartilage and formations such as protrusions and hernias.Thus, with the help of these methods, a diagnosis is accurately made, and the tomography result is an indication, and even a topical guide, for the surgical treatment of a hernia in the neurosurgery department.
Treatment of complications of osteochondrosis
Let us repeat once again that it is impossible to cure osteochondrosis, like planned aging and dehydration of the disc.You can simply not let things get complicated:
- if there are symptoms of narrowing of the height of the intervertebral discs, then you need to move correctly, not gain weight and avoid the appearance of protrusions and muscle pain;
- if you already have a protrusion, then you need to be careful not to let it rupture the fibrous ring, that is, not to transform the protrusion into a hernia, and to avoid the appearance of protrusions at several levels;
- if you have a hernia, then you need to dynamically monitor it, do regular MRIs, avoid increasing its size, or carry out modern minimally invasive surgical treatment, since without exception, all conservative methods of treating exacerbation of osteochondrosis leave the hernia in place, and only eliminate temporary symptoms: inflammation, pain, shooting and muscle spasms.
But with the slightest violation of the regime, with heavy lifting, hypothermia, injury, weight gain (in the case of the lower back), the symptoms return again and again.We will describe how you can cope with unpleasant sensations, pain, and limited mobility in the back against the background of exacerbation of osteochondrosis, and an existing protrusion or hernia, secondary to social tonic syndrome.
What to do during an exacerbation?
Since there has been an attack of acute pain (for example, in the lower back), then you need to follow the following instructions at the pre-medical stage:
- completely eliminate physical activity;
- sleep on a hard one (orthopedic mattress or hard sofa), eliminating sagging of the back;
- it is advisable to wear a semi-rigid corset to prevent sudden movements and “distortions”;
- You should place a massage pillow with plastic needle applicators on your lower back, or use a Lyapko applicator.You need to keep it for 30 - 40 minutes, 2 -3 times a day;
- after this, ointments containing NSAIDs, ointments with bee or snake venom can be rubbed into the lower back;
- after rubbing, on the second day you can wrap your lower back in dry heat, for example, a belt made of dog hair.
A common mistake is warming up on the first day.This could be a heating pad, bath procedures.At the same time, the swelling only intensifies, and the pain along with it.You can warm only after the “highest point of pain” has passed.After this, heat will enhance the “resorption” of the swelling.This usually happens on 2–3 days.
The basis of any treatment is etiotropic therapy (elimination of the cause), and pathogenetic treatment (affecting the mechanisms of the disease).It is accompanied by symptomatic therapy.For vertebrogenic pain (caused by problems in the spine), things are like this:
- In order to reduce swelling of the muscles and spine, a salt-free diet and limiting the amount of fluid consumed are indicated.You can even give a tablet of a mild potassium-sparing diuretic;
- in the acute phase of lumbar osteochondrosis, short-term treatment can be carried out with intramuscular “injections” of NSAIDs and muscle relaxants: daily.This will help relieve swelling of the nervous tissue, eliminate inflammation, and normalize muscle tone;
- in the subacute period, after overcoming the maximum pain, “injections” should no longer be taken, and attention should be paid to restorative agents, for example, modern drugs of group “B”.They effectively restore impaired sensitivity, reduce numbness and paresthesia.
Physiotherapeutic measures continue, the time has come for exercise therapy for osteochondrosis.Its task is to normalize blood circulation and muscle tone, when swelling and inflammation have already subsided, but muscle spasm has not yet completely resolved.
Kinesiotherapy (movement treatment) involves doing therapeutic exercises and swimming.Gymnastics for osteochondrosis of the cervical spine is not aimed at the discs at all, but at the surrounding muscles.Its task is to relieve tonic spasm, improve blood flow, and also normalize venous outflow.This is what leads to a decrease in muscle tone, a decrease in the severity of pain and stiffness in the back.
Exercises for osteochondrosis must be carried out after a light general warm-up, on “warmed up muscles”.The main therapeutic factor is movement, not the degree of muscle contraction.Therefore, in order to avoid relapse, the use of weights is not allowed; a gymnastic mat and a gymnastic stick are used.With their help, you can effectively restore range of motion.
Rubbing in ointments and using the Kuznetsov applicator continues.Swimming, underwater massage, Charcot shower are shown.It is during the stage of fading exacerbation that drugs for home magnetic therapy and physiotherapy are indicated.
Usually treatment takes no more than a week, but in some cases, osteochondrosis can manifest itself with such dangerous symptoms that surgery may be necessary, and urgently.
About Shants' collar
In the early stages, during the acute stage, it is necessary to protect the neck from unnecessary movements.The Shants collar is great for this.Many people make two mistakes when purchasing this collar.They do not choose it according to their size, which is why it simply does not perform its function and causes a feeling of discomfort.

The second common mistake is wearing it for prophylactic purposes for a long time.This leads to weak neck muscles, and only causes more problems.For a collar, there are only two indications under which it can be worn:
- the appearance of acute pain in the neck, stiffness and pain spreading to the head;
- if you are going to engage in physical work while in full health, in which there is a risk of “straining” your neck and getting an aggravation.This is, for example, repairing a car, when you lie down under it, or washing windows, when you need to reach out and take awkward positions.
The collar should be worn for no more than 2–3 days, since longer wearing can cause venous congestion in the neck muscles, at a time when it is time to activate the patient.An analogue of the Shants collar for the lower back is a semi-rigid corset purchased at an orthopedic salon.
Surgical treatment or conservative measures?
It is advisable that each patient, after progression of symptoms, in the presence of complications, undergo an MRI and consult a neurosurgeon.Modern minimally invasive operations make it possible to safely remove fairly large hernias, without prolonged hospitalization, without being forced to lie down for several days, without compromising the quality of life, since they are performed using modern video endoscopic, radio frequency, laser technology or using cold plasma.You can evaporate part of the kernel and lower the pressure, reducing the risk of getting a hernia.And you can eliminate the defect radically, that is, by getting rid of it completely.
There is no need to be afraid to operate on hernias; these are no longer the previous types of open operations of the 80-90s of the last century with muscle dissection, blood loss and a subsequent long recovery period.They are more like a small puncture under X-ray control followed by the use of modern technology.
Prevention of osteochondrosis and its complications
Osteochondrosis, including complicated ones, the symptoms and treatment of which we discussed above, is for the most part not a disease at all, but simply a manifestation of inevitable aging and premature “shrinkage” of the intervertebral discs.Osteochondrosis needs little to never bother us:
- avoid hypothermia, especially in autumn and spring, and falls in winter;
- do not lift weights, and carry loads only with a straight back, in a backpack;
- drink more clean water;
- don’t get fat, your weight should correspond to your height;
- treat flat feet, if any;
- do physical exercises regularly;
- engaging in types of exercise that reduce the load on the back (swimming);
- giving up bad habits;
- alternating mental stress with physical activity.After every hour and a half of mental work, it is recommended to change the type of activity to physical work;
- You can regularly do at least an x-ray of the lumbar spine in two projections, or an MRI, to know whether the hernia, if any, is progressing;
By following these simple recommendations, you can keep your back healthy and mobile for life.